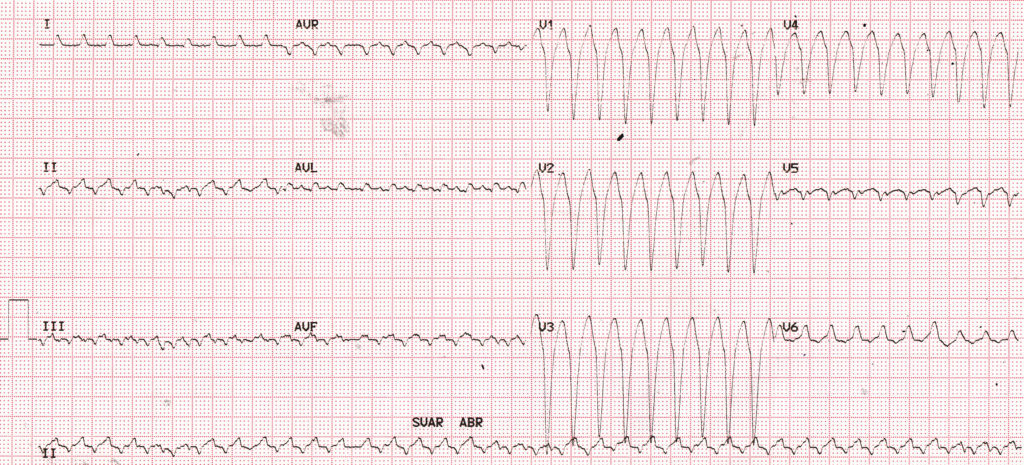
What are the possibilities in this wide QRS tachycardia?
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
7 Comments
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
Vt
12 lead standard electrocardiogram showing regular wide complex tachycardia.
Differentials are 1. VT with two different morphologies which itself is against VT.
2. AVNRT with aberrancy
3.AVRT
I will say AVNRT with aberrancy because we cannot explain two pathologies from AVRT or VT.AVNRT with conduction pathway explain both the findings.
Finding favour VT- No rs morphology, fusion beats and left axis deviation.
My final answer AVNRT with aberrancy.
Flutter with 1:1 . To fast for VT, I think.
There is a classic LBBB morphology here which leads me to think in terms of a supraventricular rhythm. The rhythm is fairly regular with one exception: there is a missing beat following the 12th QRS. Since the rhythm continues without being reset, this would represent a Mobitz II block which essentially rules out AVNRT or AVRT with aberrancy since a block in either one should terminate the dysrhythmia. However, an automatic or reentrant ectopic site (as opposed to AVNRT or AVRT) could experience a momentary exit block. No P waves are visible so this may represent a junctional tachycardia with aberrancy or ventricular tachycardia (even though the QRS complexes look classic for LBBB). Another problem is then raised: the mean QRS axis takes a 180 degree shift in the 5th and 6th QRS complexes (and later in the strip). This could be due to more than one exit site in an automatic or reentrant ectopic pacemaker. It could also be due to a change to a momentary shift to another fascicle in the left ventricle. Here are my possibilities:
1. Junctional tachycardia with aberrancy
2. VT (automatic or reentrant)
vt , syt with aberration
, preexcited afib
1. JET with aberrancy
2. VT
Look at lead 2 rhythm stip,the negative P is missing in some beats, this rule out AVNRT or ANRT. But can be explained by blocked VA conduction in VT or JET.
The changing of QRS morphology in a few beats could be explained by fusion or capture beats in VT. Or capture beats in JET.
VT with Lbbb morphology with superior axis.. Most commonly due to ARVD