What are the possibilities in this wide QRS tachycardia? – Discussion
What are the possibilities in this wide QRS tachycardia?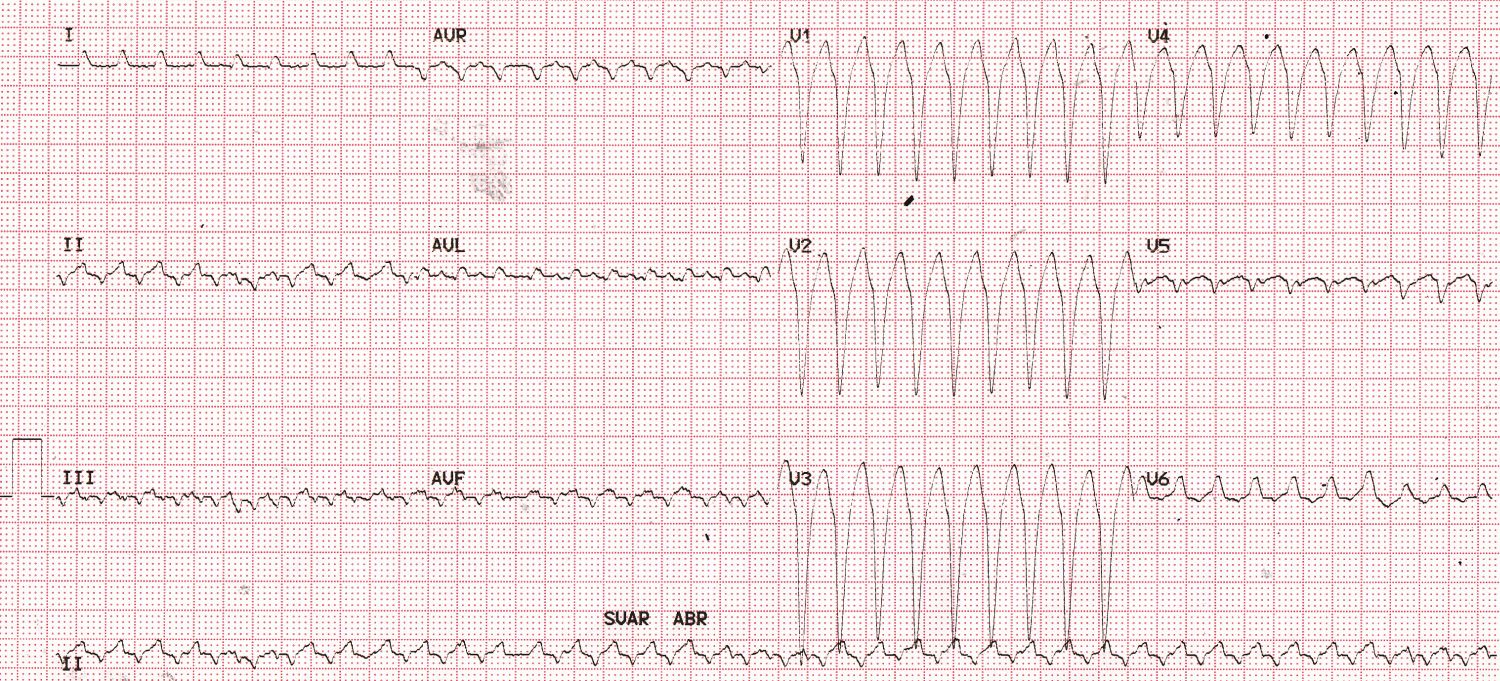
Wide QRS tachycardia – Discussion
Wide QRS complex tachycardia with a rate of around 225/min. Wide QRS tachycardia is to be taken as ventricular tachycardia until proved otherwise. Monophasic negative wide QRS complexes are seen from V1-V5. V6 shows positive wide QRS complex with LBBB morphology. Similar morphology is seen in leads I and aVL as well. The QRS voltages are low in limb leads. Lead II shows multiple irregularities in baseline which could be dissociated P waves. The atrial rate calculated from the dissociated P waves seems to similar to that of the tachycardia rate, though one can’t be very sure as to which irregularities are P waves and which are artifacts!
Atrial flutter with 1:1 conduction and aberrant ventricular conduction is another possibility to be considered with a fast rhythm. But the usual rate of atrial flutter waves is 300/min, unless the flutter has been slowed by some other mechanism. Presence of dissociated P waves is against the diagnosis of atrial flutter. Other types of supraventricular tachycardia with aberrancy of ventricular conduction are also excluded by the same feature.
Discussion on very fast wide QRS tachycardia: Ventricular tachycardia is considered to be very fast if the cycle length is between 200 to 230 ms. Zaman S and associates noted that majority of inducible ventricular tachycardias in patients who have been reperfused early for ST segment elevation myocardial infarction are very fast. They noted that these inducible fast ventricular tachycardias have at least a similar risk or arrhythmia or death as inducible standard ventricular tachycardia with cycle length more than 230 ms [1].
Reference
- Zaman S, Kumar S, Sullivan J, Narayan A, Thiagalingam A, Ross DL, Kovoor P. Significance of inducible very fast ventricular tachycardia (cycle length 200-230 ms) after early reperfusion for ST-segment-elevation myocardial infarction. Circ Arrhythm Electrophysiol. 2013 Oct;6(5):884-90.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
VT but possibility of PAT with aberrant conduction.