Treadmill Exercise ECG (TMT)
Treadmill Exercise ECG (TMT)
Treadmill Exercise ECG, also known as treadmill test (TMT) and stress ECG is usually done with a computerized treadmill unit which controls the motor speed of the treadmill as well as monitors the ECG. ECG is recorded periodically during the test in addition to documenting any specific events like arrhythmias. The treadmill test is done in a basal state (fasting) so that the process of digestion of food and consequent increase in cardiac output does not interfere with the assessment. If it is a diagnostic test, the individual should be off medications. But if it is for assessment of effort tolerance while on treatment, it may sometimes be done on medications.
Though various protocols like Naughton and ramp protocol are in vogue, the popular one is Bruce protocol. There is also a Modified Bruce protocol for those with lower functional capacity or for early post infarction evaluation. Standard Bruce protocol has seven 3 minute stages. In stage I the gradient is 10% and it rises 2% per stage. The starting speed is 1.7 mph and increases in increments of 0.8 to 0.9 mph per stage. In Modified Bruce protocol, stage I has a gradient of zero and stage II a gradient of 5%. Speed is the same in the first 3 stages of Modified Bruce protocol (1.7 mph). Stage 3 of Modified Bruce protocol is equivalent to Stage I of standard Bruce protocol. Further stages are similar to Bruce protocol, though the number of the stage will be higher by a magnitude of 2.
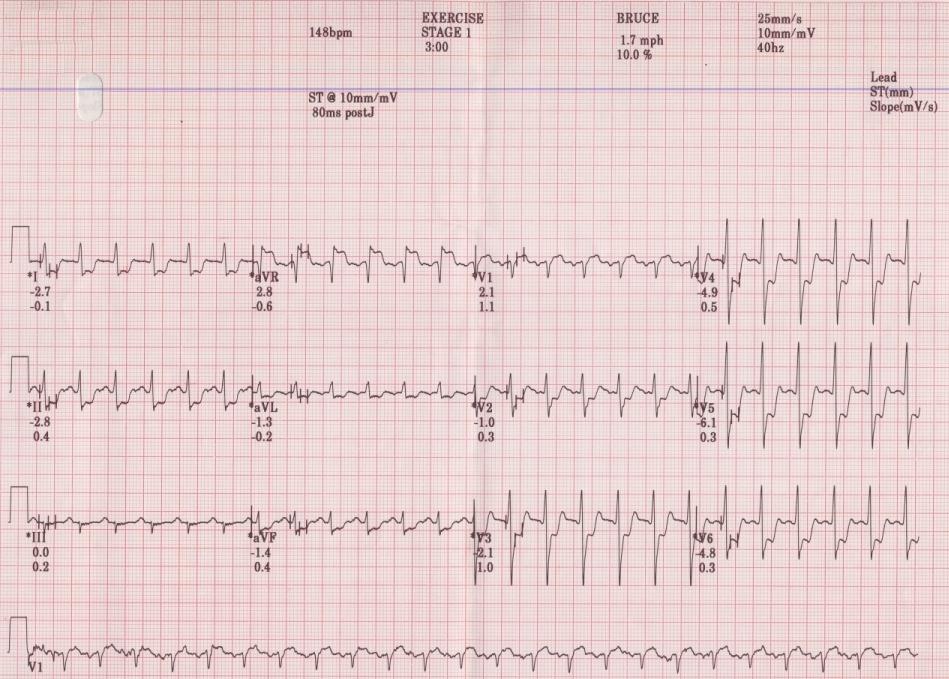
Strongly positive TMT showing deep ST depression in inferior and anterolateral leads, with ST segment elevation in aVR and V1, in stage I.
Basal metabolic requirement is taken as 1 MET (metabolic equivalent) which is equivalent to 3.5 ml/kg/minute of oxygen consumption. If stage I of Bruce protocol is completed, 4.6 METS are achieved. For stage II it is 7.0 and 10.1 for stage III. The treadmill speeds at these stages are 1.7, 2.5 and 3.4 mph respectively. For stage IV the speed is 4.2 mph.
The most important change noted in the treadmill test is the ST segment depression as seen in the illustration. If it occurs in Stage I of standard Bruce protocol and if it is severe, it is a strongly positive TMT as in the illustration. The lower the workload at which the ST segment depression occurs, the more likely the person is to have severe coronary artery disease. ST segment depression occurring within 5 minutes of Bruce protocol and persisting more than 5 minutes into recovery is highly significant. ST segment depression can be upsloping, horizontal or down sloping, in the order of significance. An upsloping ST segment depression can be normal if it is a rapid upsloping ST, which is said to represent the atrial repolarization wave (Ta wave) extending into the region of the ST segment with exercise. ST segment depression is measured at 80 ms from the J point (end of QRS) at heart rates below 120/min and at 60 ms at higher heart rates.
ST segment elevation has the same significance as ST segment depression in leads not showing an initial Q wave. In those leads with a Q wave, it can be due to dyskinesia or left ventricular aneurysm [1-3]. It is can also be a feature of viable myocardium in an infarcted territory, with poor collateralization [2]. Hibernating myocardium has been invoked as a reason by Malouf D et al as their patient had resolution of wall motion abnormalities after revascularization [4].
Coronary spasm is another potential cause of ST elevation during treadmill exercise ECG. In one study, 12 patients without history of myocardial infarction or left ventricular aneurysm, had provocation of coronary spasm with ergonovine [5].
References
- Chahine RA, Raizner AE, Ishimori T. The clinical significance of exercise-induced ST-segment elevation. Circulation. 1976doi: 10.1161/01.cir.54.2.209. PMID: 939022.
- Miyakoda H, Kato M, Noguchi N, Omodani H, Osaki S, Matsumoto T, Kinugawa T, Hoshio A, Kotake H, Mashiba H. Exercise-induced ST-segment elevation–role of left ventricular wall motion abnormalities and coronary artery narrowing. Jpn Circ J. 1995 Nov;59(11):725-35.
- Macieira-Coelho E, Garcia-Alves M, Dionisio I, Cantinho G, Da Costa BB, Gouveia A. Role of myocardial ischemia and left ventricular wall motion abnormalities as contributory factors in the genesis of exercise-induced ST-segment elevation in Q-wave myocardial infarction. Cardiology. 1999;91(4):227-30.
- Malouf D, Mugmon M. ST elevation occurring during stress testing. J Community Hosp Intern Med Perspect. 2016 Apr 25;6(2):30799.
- Specchia G, de Servi S, Falcone C, Angoli L, Mussini A, Bramucci E, Marioni GP, Ardissino D, Salerno J, Bobba P. Significance of exercise-induced ST-segment elevation in patients without myocardial infarction. Circulation. 1981 Jan;63(1):46-53.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal