Tight discrete right coronary artery lesion
Tight discrete right coronary artery lesion
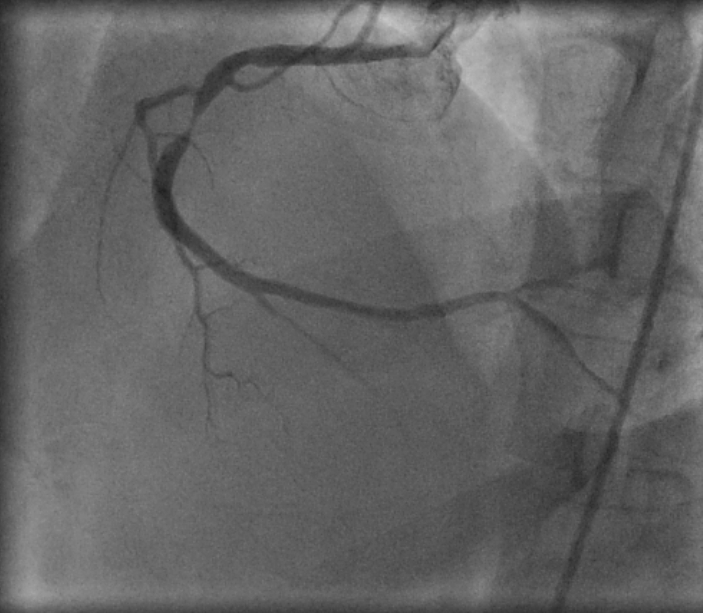
Coronary angiogram using a Judkins right coronary catheter showing a tight discrete right coronary artery lesion just distal to a right ventricular branch. The distal vessel is good, with a suspicion of mild lesion at the bifurction of RCA into posterior descending coronary artery and posterior left ventricular branch. The proximal lesion appears to be a good target for percutaneous intervention. Apparently, it should be easy to cross as a lumen is still visible and the side branch is not arising at the site of the lesion.
If the side branch was arising from the site of the lesion and was more parallel to the lesion, the guide wire can preferentially track into the side branch rather than crossing the lesion. Here the side branch is proximal to the lesion and arises at almost a right angle to the parent vessel. But the lumen starts tapering from the region of the side branch and the side branch ostium appears hazy. Hence while stenting the flow to the side branch is likely to be compromised. As it is a small branch, there may not be much problem due to compromising the side branch flow.
Whiff of dye is seen effluxing from the right coronary ostium into the aorta and right sinus, indicating that the catheter has not been wedged within the artery. If dye reflux is not seen, there is a chance of trauma to the ostium and also ischemia due to compromise of the coronary flow. Wedging will also be manifested by damping of the catheter tip pressure tracing. Damping is quite common during angiography of small, non-dominant right coronary arteries. Occasionally the damping is because the catheter is wedged in a conus branch of the right coronary artery or a conus artery which is arising independently. In either case, the catheter has to be withdrawn quickly. Injection into the conus artery can produce ST elevation, ventricular tachycardia or even ventricular fibrillation. Sometimes the catheter can slip into the conus artery during contrast injection as well.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal