Left bundle branch block
Left bundle branch block
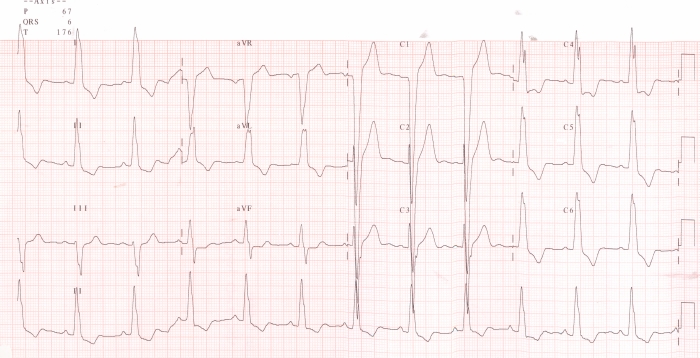
Left bundle branch block is characterised by a wide QRS complex, more than 120 ms, with tall slurred R waves in lateral leads I, aVl, V5 and V6 and QS complex in lead V1. The QS complex in V1 may have a W pattern. As the initial left to right activation is lost in left bundle branch block, the initial q wave in lateral leads and the initial r wave in right precordial leads are absent. ST segment and T wave are opposite in direction to the predominant QRS vector so that ST segment is depressed and T wave inverted in lateral leads with tall R waves. Vice versa, the ST segment is elevated and T waves upright in lead V1. This pattern is known as discordant ST segment and T wave in left bundle branch block. If the pattern becomes concordant, it is suggestive of a primary myocardial pathology like ischemia or infarction. Hence upright T wave in lateral leads in LBBB is suggestive of myocardial ischemia or infarction.
If the QRS duration is less than 120 ms with the same pattern, it is often called incomplete LBBB. If there are prominent q waves in lateral leads or r waves in V1 in LBBB, it is suggestive of associated myocardial infarction. Unlike right bundle branch block, LBBB is often associated with structural heart disease. A new onset LBBB in the setting of acute coronary syndrome was taken as equivalent to ST elevation myocardial infarction and taken as an indication for thrombolytic therapy in 2004 guidelines. But that was removed in the 2013 guidelines due to lack of specificity.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal