Hypertrophic obstructive cardiomyopathy – echocardiogram video
Hypertrophic obstructive cardiomyopathy
Echocardiogram with narration:
Echocardiogram without narration:
Hypertrophic cardiomyopathy is an autosomal dominant disorder with 50% involvement of first degree relatives, though the extent of involvement is variable. The hallmark of the disorder is severe hypertrophy of the left ventricle, even though biventricular forms may be seen rarely. In the obstructive variety of hypertrophic cardiomyopathy, asymmetric hypertrophy of the interventricular septum compared to the posterior wall is the predominant feature. The hypertrophied septum impinges on the left ventricular outflow tract producing obstruction.
Diastolic frame of echocardiography in parasternal long axis view in hypertrophic cardiomyopathy
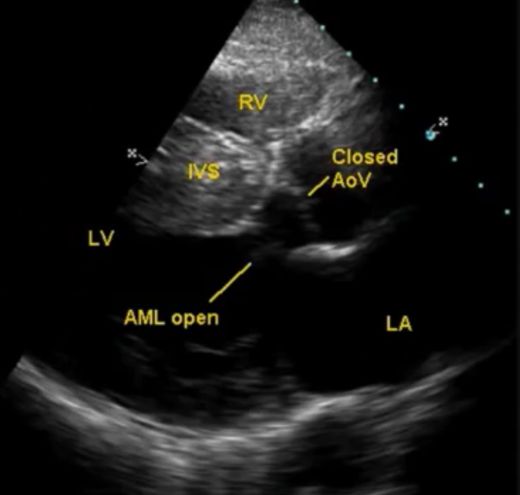
Diastolic frame of hypertrophic obstructive cardiomyopathy – echocardiogram in parasternal long axis view, demonstrating the thickened interventricular septum, (IVS) which is disproportionate to the thickness of the left ventricular posterior wall. The echodensity of the IVS is also varying, with a speckled appearance. The anterior mitral leaflet (AML) is in an open position and aortic valve (Ao V) is in a closed position, indicating diastole. LA: left atrium; RV: right ventricle; LV: left ventricle. The left atrium is dilated (compare with the aortic size – usually both are roughly equal in this view).
Mitral diastolic flow in hypertrophic cardiomyopathy

Colour Doppler evaluation (color flow mapping) in the parasternal long axis view in hypertrophic cardiomyopathy illustrating the mitral diastolic flow. Desc Ao: descending aorta. The mitral flow is not turbulent, as indicated by the blue colour without any variance or mosaic formation. The AML is seen in open position and aortic valve in closed position, suggesting diastolic frame.
Early systolic frame in echocardiography in hypertrophic cardiomyopathy
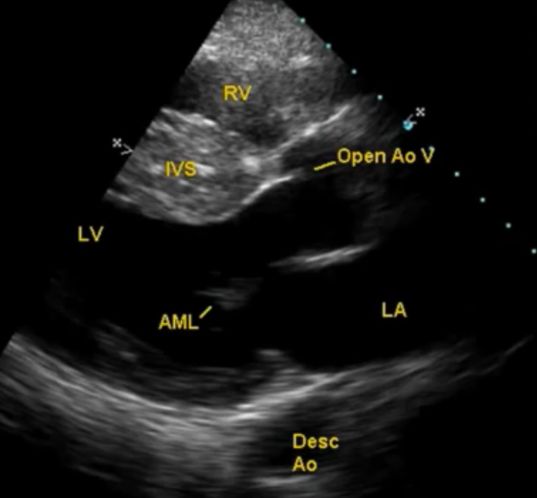
Early systolic frame shows that the aortic valve is open, but the left ventricular outflow tract (LVOT) is wide and the AML is in the closed position. This frame is just before the onset of the systolic anterior motion (SAM) of the mitral valve. In the eject – obstruct – leak sequence of dynamic LVOT obstruction, this is the initial eject phase.
Colour flow mapping in early systole in hypertrophic cardiomyopathy
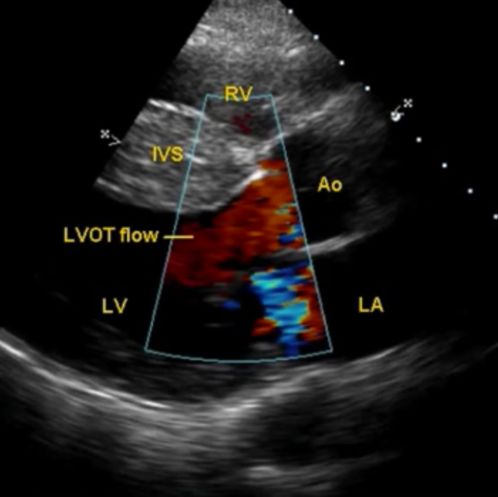
Colour flow mapping (Color Doppler imaging) in early systole in hypertrophic cardiomyopathy shows that the flow in the LVOT is not turbulent (red color without any mosaic or variance). This corresponds to the eject phase of the eject-obstruct-leak sequence. The blue color behind the mitral valve is possible a slight back flow during the closing of the mitral valve.
Systolic anterior motion (SAM) of mitral valve in hypertrophic obstructive cardiomyopathy
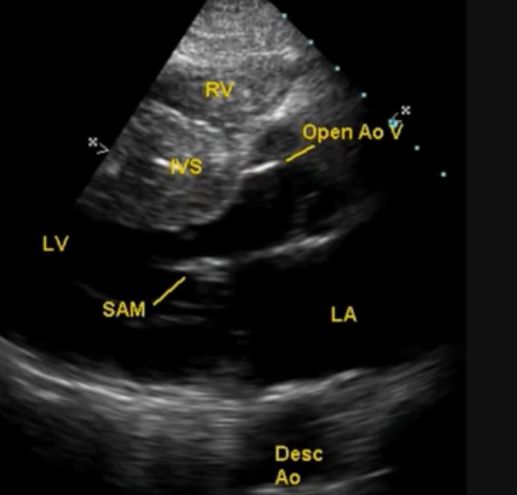
Echocardiographic frame later in systole, demonstrating the systolic anterior motion (SAM) of the mitral valve. This is due to suction effect of the LVOT ejection (Venturi effect). SAM causes further narrowing of the LVOT, in addition to the obstruction caused by the hypertrophied septum jutting into the LVOT. Abnormal orientation of the papillary muscle and the consequent pull can also contribute to the SAM.
SAM septal contact time is the time during which the SAM touches the IVS. The more the SAM septal contact time, the more severe the LVOT obstruction. SAM septal contact also causes the formation of a plaque in this region, which could be a nidus for infective endocarditis in hypertrophic cardiomyopathy (HCM). Another site for vegetations in HCM is the aortic valve on which the LVOT jet strikes, usually the ventricular aspect.
Hypertrophic obstructive cardiomyopathy with turbulent LVOT flow and mitral regurgitation by CFM
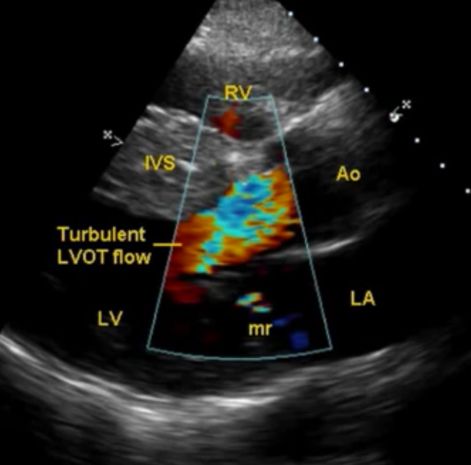
Colour flow mapping (CFM) during the SAM shows turbulent flow in the LVOT. A small mitral regurgitation (mr) jet is also visible behind the mitral valve, into the left atrium. This image demonstrates the last two phases of the eject-obstruct-leak sequence in hypertrophic obstructive cardiomyopathy. Dynamic changes in LVOT obstruction can be brought out by giving and releasing hand grip as well as imaging in the supine and standing position. But imaging in standing position is difficult as the echo window will not be good in the standing position. Still it might be possible to demonstrate dynamic changes in the gradient in certain cases.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal