ECG in hyperkalemia
ECG in hyperkalemia
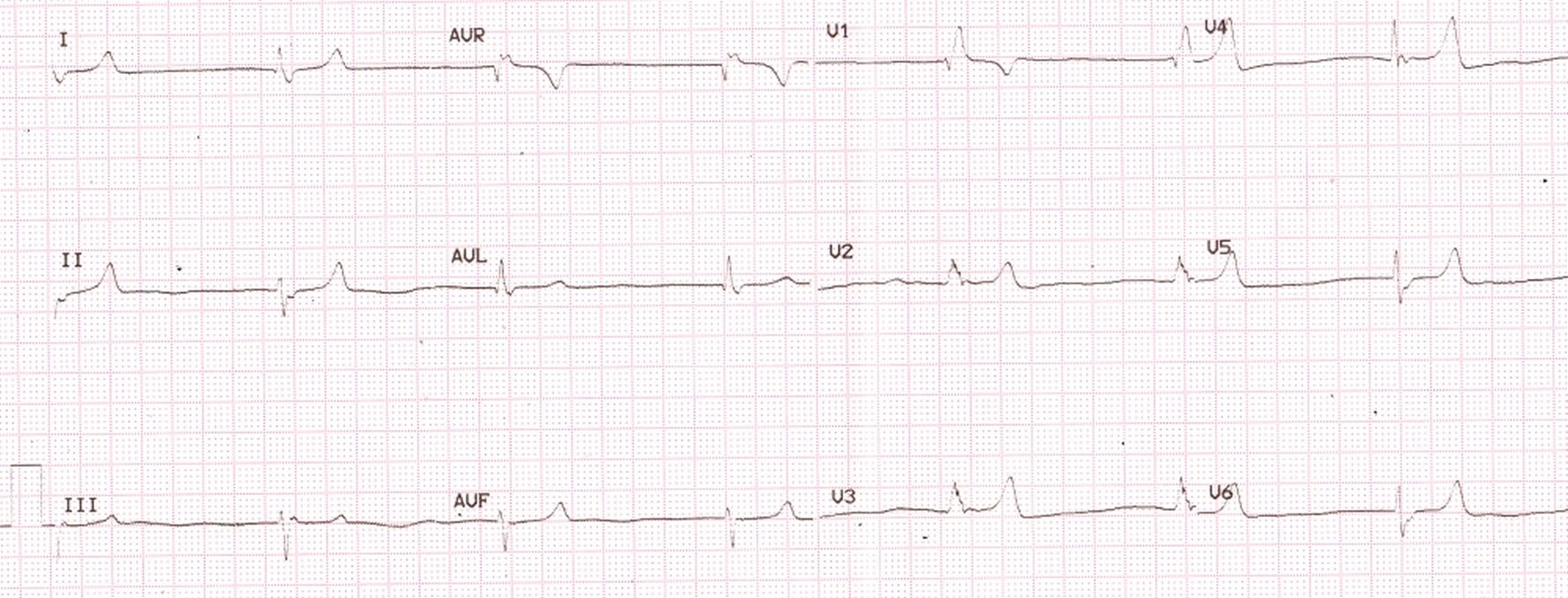 In this ECG some features due to hyperkalemia are visible:
In this ECG some features due to hyperkalemia are visible:
- Tall T waves – T waves in anterior leads are as tall as or taller than the QRS complexes, though the absolute amplitudes are not very high. Typical description in hyperkalemia is tall tented T waves.
- QRS widening, with right bundle branch block like pattern
- Lack of atrial electrical activity – no P waves are visible and there is bradycardia. It could very well be a slow junctional rhythm. Ideally if there was sinus arrhythmia visible in the QRS complex intervals, one could have presumed that there is sinus node activity with atrial paralysis and sinoventricular conduction [1].
In severe hyperkalemia, QRS becomes very wide and merges with T wave to produce a sine wave pattern (not seen in the ECG illustrated above) in which there will be no visible ST segment [2]. In the case reported by Pluijmen MJ et al [2], the patient was hemodynamically stable, but presented with quadriplegia, had heart rate 45/min and had end stage renal disease. Serum potassium was 9.9 mmol/L. Intravenous calcium gluconate was given and emergency dialysis performed. Sinus rhythm was maintained once normokalemia was achieved.
References
- Maradey J, Bhave P. Sinoventricular Conduction in the Setting of Severe Hyperkalemia. JACC Clin Electrophysiol. 2018 May;4(5):701-703.
- Pluijmen MJ, Hersbach FM. Images in cardiovascular medicine. Sine-wave pattern arrhythmia and sudden paralysis that result from severe hyperkalemia. Circulation. 2007 Jul 3;116(1):e2-4.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal