ECG in cardiac resynchronization therapy (CRT)
ECG in cardiac resynchronization therapy (CRT)
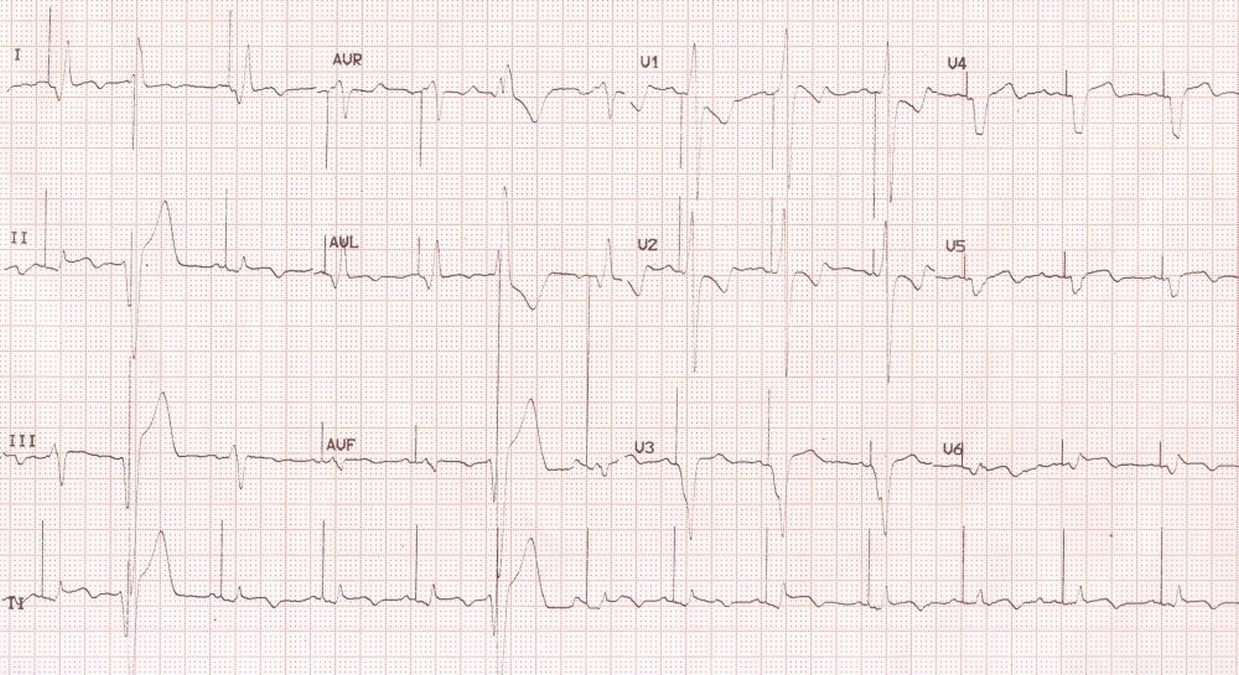
While evaluating an ECG in cardiac resynchronization therapy (CRT, biventricular pacing), we have to decide whether the device is capturing both ventricles or only one ventricle. In lead I a positive QRS is indicative of right ventricular (RV) pacing while biventricular (BV) pacing shows a negative QRS, almost like an inverted pattern compared to RV pacing. In the complexes 1 and 3 in lead I in the current ECG, the pattern is suggestive of RV pacing. The presence of an R wave in V1 indicates that there is definitely a contribution from left ventricular pacing. Complex 2 looks an ectopic beat over which a pacing artefact is superimposed. Though it may appear to be pseudofusion, it is more likely to be safety pacing in CRT-D. The large pacing artefacts suggests that it is a unipolar pacing mode. The AV interval is quite short (120 msec) and the atria are being tracked well. The paced QRS complexes have a leftward axis. Width of the paced QRS (120 msec) also suggest that it is univentricular pacing rather than BV pacing. Leads I, II and III are most useful in deciding whether it is RV, LV (left ventricle) or BV pacing. Since the pattern varies from individual to individual, it is good to preserve the tracings of all modes of pacing for future comparison. Changes in paced complexes, in particular of the BV and LV complexes may indicate possible LV lead displacement.
If you wish to see and X-ray chest PA view in cardiac resynchronization therapy, please click on the link.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal