Ebstein’s anomaly of tricuspid valve
Ebstein’s anomaly of tricuspid valve
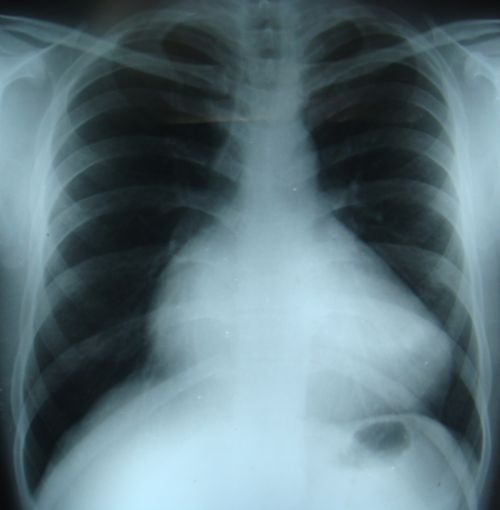
X-ray chest PA view in Ebstein’s anomaly of tricuspid valve showing cardiomegaly with prominent right atrial enlargement. Right atrial enlargement is seen as enlargement of the cardiac contour to the right side of the spine, usually more than 5 cm from the midline. Cardiomegaly with relative oligemia of the lung fields and reduced cardiac motion can produce a “stencilled out” appearance in Ebstein’s anomaly.
In Ebstein’s anomaly, the tricuspid valve attachment is displaced distally so that the septal and posterior leaflets are attached more distally in the right ventricle rather than at the atrioventricular junction. The anterior leaflet which is not displaced is large, sail like and produces a “sail sound” while closing (loud T1 or tricuspid component of first heart sound). A portion of right ventricle is “atrialized” due to the distal attachment of tricuspid leaflets. Hence the right ventricle is small and right atrium very large in Ebstein’s anomaly. Cyanosis is common in Ebstein’s anomaly due to right to left shunt at the atrial level. Right to left shunt in Ebstein’s anomaly is not due to pulmonary hypertension, but due to the direction of the tricuspid regurgitation jet towards the left atrium. Auscultatory hallmarks of Ebstein’s anomaly are multiple heart sounds, loud T1 or sail sound and a scratchy, superficial diastolic murmur due to tricuspid stenosis.
The large right atrium and an association of right sided accessory pathways make Ebstein’s anomaly prone for supraventricular tachycardias. Localization and ablation of accessory pathways in Ebstein’s anomaly is difficult due to the large right atrium and distorted anatomy. The atrialized portion of right ventricle will show ventricular electrograms and an atrial pressure tracing. This is known as Hernandez sign. Hernandez sign is elicited using a catheter which can record electrogram as well as measure the pressure known as Zucker catheter.
ECG in Ebstein’s anomaly is characterised by tall P waves due to right atrial enlargement and splintered QRS in V1, which mimics a right bundle branch block pattern, but is polyphasic. Features of right sided accessory pathways can also be noted in Ebstein’s anomaly. Sometimes the ECG may manifest reentrant atrioventricular tachycardia (AVRT).
Ebstein’s type of anomaly of the left atrioventricular valve is seen in levo transposition of great arteries (congenitally corrected transposition, L-TGA, cTGA).
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal