Coronary CT (computerised tomography) angiography
Coronary CT (computed tomography) angiography
Multi slice CT for coronary artery imaging
Multi slice CT (MSCT) scanners are becoming popular as a non-invasive imaging modality for screening coronary artery disease. The era of MSCT started with 4 slice scanners and progressed to the 64 slice MSCT which is commonly used now. 256 slice and 320 slice CT scanners are also being evaluated for clinical use. One of the difficulties with cardiac CT for imaging coronaries is the constant motion of the heart. This can be partly overcome by using ECG gating of the signals. Conventionally this has been done by retrospective ECG gating. This would mean that CT data is acquired through out the cardiac cycle and only those signals during a particular part of the cardiac cycle, usually a diastolic frame is used for final reconstruction of the coronaries. This would mean a much higher dose of radiation. Now prospective ECG gating is being evaluated in MSCT to reduce the radiation dose so that data acquisition is done only during the selected phase of the cardiac cycle. Prospective ECG gating can reduce the radiation dose up to 90% as compared to retrospective ECG gating. But the quality of images will come down if the heart rate or heart rate variability is high in prospective ECG gating. So also, higher body mass index (BMI) also causes lower image quality. Prospective gating can cause stair step artefacts due to patient motion on the CT table as multiple acquisitions may be needed to cover the z-axis with 64 slice CT. This is avoided in 320 slice CT as the gantry can cover the whole heart in one cycle due to better z-axis coverage. Dual source CT also gives better results.
Imaging of the coronaries is ideally done at lower heart rates and beta blockers are often administered to lower the heart rate during MSCT if the basal heart rate is high. As the number of slices increased, the resolution of the system to pick up more and more details of the coronary anatomy has improved. Main coronary arteries as well as side branches can be visualized well with ECG gated 64 slice CT. 320 slice CT will improve the quality of images further. The whole imaging can be completed in one cardiac cycle, even with prospective ECG gating. This would mean that patients with cardiac arrhythmias are no longer excluded from cardiac CT evaluation of the coronaries.
64-Slice computed tomography angiography has a high sensitivity and negative predictive value
64-Slice computed tomography angiography as diagnostic tool in coronary artery disease has been evaluated in a meta analysis by Mowatt et al (Heart 2008;94:1386-1393). Of the 40 studies identified, 28 had sufficient data for inclusion in the meta analysis. The studies included were those comparing 64-Slice computed tomography angiography with standard coronary angiography. The pooled data offered a sensitivity of 99% and specificity of 89% taking 50% or more coronary stenosis as a cut off point. The median positive predictive value across studies was 93% (range 64–100%) and negative predictive value 100% (range 86–100%).
The authors suggest that 64-Slice computed tomography angiography may have a role in the assessment of undiagnosed chest pain when simple non-invasive investigations are non-diagnostic and can rule out significant coronary artery disease in this context.
Cardiac CT images of coronary arteries
Cardiac CT scan image of LCX
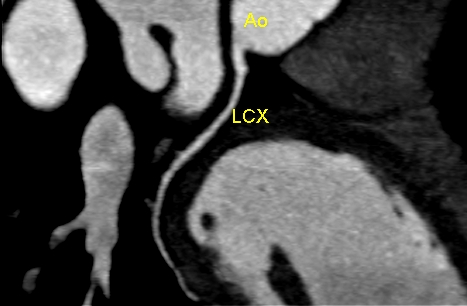
Cardiac CT scan image of left circumflex (LCX) coronary artery in the atrioventricular (AV) groove, seen arising from the aorta (Ao). Hence caution has to be exerted before committing that a short segment visualized is the stump of an occluded artery as the segments may become invisible when the plane of imaging changes in tomographic images.
Normal cardiac CT images: Coronaries on reconstructed views
Cardiac CT angiograms are increasing in popularity as a non-invasive screening tool for detecting significant coronary artery disease. The angiograms are reconstructions from 64 or more slice CT scans following intravenous injection of radiocontrast dye. As of now it cannot replace conventional coronary angiograms for assessing the detailed coronary anatomy.

LAD, LCX and Left main on reconstructed cardiac CT
Reconstructed cardiac CT scan image as viewed from the left anterior aspect, showing left main coronary artery (LM), left circumflex (LCX) coronary artery and left anterior descending (LAD) coronary artery. Ao: aorta. Two diagonal branches are also seen arising from the LAD. LCX is occupying the atrioventricular (AV) groove.

LMCA, LAD, LCX and coronary sinus on reconstructed cardiac CT
Reconstructed cardiac CT image as viewed from the posterior aspect showing the left anterior descending (LAD) coronary artery, left main coronary artery (LMCA), left circumflex (LCX) coronary artery and the coronary sinus (Coron sinus). The main tributaries of the coronary sinus are also seen joining it. A diagonal branch is seen arising from the LAD and an obtuse marginal branch from the LCX (not marked).
 RCA in the AV groove on reconstructed cardiac CT
RCA in the AV groove on reconstructed cardiac CT
Reconstructed cardiac CT image showing the right coronary artery (RCA) in the atrioventricular (AV) groove. The left anterior descending (LAD) coronary artery is seen to the left extreme of the image, though it is not visualized well. A diagonal branch of the LAD is also visible.

Distal RCA and coronary sinus on reconstructed cardiac CT
Distal right coronary artery (RCA) and coronary sinus seen in the atrioventricular (AV) groove seen on the posterior aspect view of reconstructed cardiac CT. Left circumflex coronary is seen adjacent the coronary sinus in the AV groove.
Uninterpretable risk score for coronary CT angiography
Coronary CT angiography (CCTA) is being used increasingly as a screening tool for coronary artery disease (CAD) in those with an intermediate or low risk for CAD. Acquisition of good quality images is an important factor in the success of coronary CT angiography. But in some individuals, this may not be possible due to various reasons. Vanhecke TE and associates {Vanhecke TE et al. Development and Validation of a Predictive Screening Tool for Uninterpretable Coronary CT Angiography Results. Circ Cardiovasc Imaging. 2011 Jul 20. [Epub ahead of print]} have developed an uninterpretable risk score using clinical and patient variables. They identified variables which were independently associated with the occurrence of at least one uninterpretable major coronary segment, using data from over eight thousand five hundred patients. This was then prospectively validated among nine hundred odd patients. The scores ranged from zero to twelve. The risk score was predictive of uninterpretable results in both the development and validation cohorts used in the study. The seven factors which constitute the uninterpretable risk score are diabetes mellitus, hypertension, chronic obstructive pulmonary disease (COPD), sedentary lifestyle, body mass index, age, and history of atrial fibrillation. The authors conclude that the scoring system may help in predicting those in whom the unnecessary radiation exposure due to the study may be avoided if the risk score suggests uninterpretable results.
Risk of coronary event with non obstructive plaques
Non obstructive coronary plaques do not need percutaneous coronary interventions, but some of them may lead on to acute coronary events later on. The calcified plaques may not lead on to events, but the vulnerable plaques with a lipid rich core and a thin fibrous cap are the ones prone for fissuring of the cap or rupture which leads an intracoronary thrombus formation and a consequent acute coronary event.
Kristensen TS and associates [Kristensen TS et al. Prognostic Implications of Nonobstructive Coronary Plaques in Patients With Non–ST-Segment Elevation Myocardial Infarction. A Multidetector Computed Tomography Study. J Am Coll Cardiol, 2011; 58:502-509] evaluated non obstructive coronary plaques in those with non ST elevation myocardial infarction and followed them up. Over three hundred patients were underwent 64 slice multidetector computed tomography (MDCT) coronary angiography and coronary artery calcium scoring before conventional coronary angiography. Plaque composition and volume were measured quantitatively for all non obstructive coronary lesions. Standard guideline based invasive treatment was given. Twenty three patients had a cardiac event at a median follow up of sixteen months. Increasing amount of non calcified plaque was associated with age, male sex and diabetes mellitus. Total volume of non calcified plaque was independently associated with an increased hazard ratio. But Agatston score or the amount of calcium in the non obstructive lesions were not associated with increased risk.
Multicolor CT and gold nanoparticles for evaluation of plaque
Multicolor CT is the popular name for spectral computed tomography. In spectral CT system, the incident x-rays are divided into multiple energy bins and is used for multicolor imaging. Gold high density nanoparticle contrast agent (Au-HDL) can be used for characterization of macrophage burden as they are taken up by the macrophages in the atherosclerotic plaques. A recent study published in Radiology. 2010 Sep;256(3):774-82 by Cormode DP et al evaluated the use of gold nanoparticles along with multicolor CT in animal studies of atherosclerotic plaques. Multi color CT enabled differentiation of gold nanoparticles, iodine based contrast and calcium phosphate. Gold nanoparticles were located primarily in the macrophages in the aortic sections. This combined imaging enabled characterization of stenosis by the plaques, calcification and the macrophage burden. Macrophage rich plaques are considered as vulnerable plaques prone for rupture and producing vascular events like acute coronary syndrome.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal