Supraventricular ectopics
Supraventricular ectopics
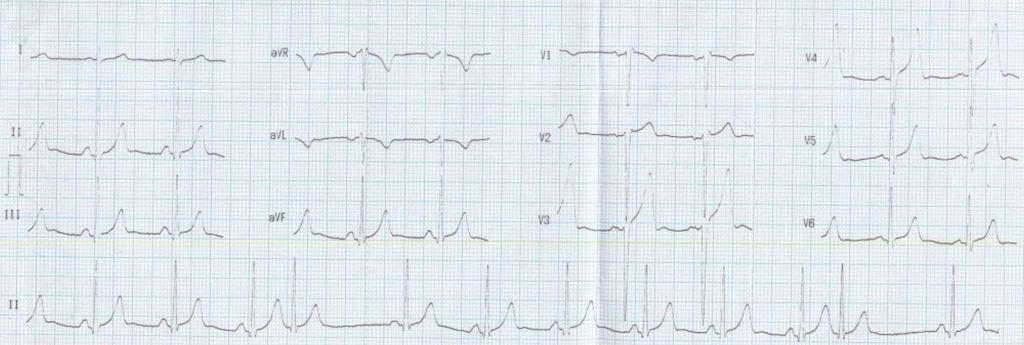
Lead II rhythm strip at the bottom of the images show two premature complexes (4th and 11th). These premature complexes are narrow and resemble the QRS complexes of sinus rhythm. Hence they are supraventricular ectopic beats. Ventricular ectopic beats are bizarre and wide, totally different from the QRS complexes in sinus rhythm. Supraventricular ectopic beats originating in the atrium or upper part of the AV junction have P waves preceding the QRS complexes. But these may be submerged in the T wave of the preceding beat.
Mid junctional beats have their P waves within the QRS complex and hence obscure. In a low junctional rhythm inverted P waves can be seen after the QRS with a short RP interval. In the current tracing, no definite P waves belonging to the ectopic beat are discernible. The premature beat is followed by a compensatory pause which is less than fully compensated in that it is about 120 msec less than twice the regular sinus cycle length. In ventricular ectopic beats, the pauses are fully compensatory meaning that the coupling interval between the preceding normal beat and the ectopic beat added to the pause will be exactly twice the regular sinus cycle length.
This is because the ventricular ectopic beat seldom gets conducted back to the sinus node to reset it or it reaches there late after the sinus beat has already occurred and captured the atrium. In contrast, the supraventricular ectopic beat usually discharges the sinus node prematurely and resets the sinus cycle so that the pause is less than fully compensated. The difference in the length of the pause from the sinus cycle length depends on the time taken for the supraventricular ectopic beat to travel upto the region of the sinus node, at which point the sinus cycle restarts. The pause can be lengthier if there is suppression of the sinus node activity by the ectopic discharge as in sinus node dysfunction.
This ECG also shows deep S waves in V2 and V3 which might indicate left ventricular hypertrophy. The tall T waves in V3 and V4 is more of a normal variant than that which could occur in hyperkalemia and hyperacute phase of myocardial infarction. The latter condition is often missed and mandates a repeat ECG if the clinical condition is suggestive.
Related Posts



About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal